
Why Can't I Get Aroused?

“Is that a gun in your pocket, or are you just happy to see me?”
Mae West
What Do We Mean By Arousal?
Arousal is something exciting, something yummy, something juicy, that gets us breathing a little quicker and makes our eyes sparkle.
- But what actually is going on when we get aroused?
- How does it work?
- And what can we do if it’s not working the way we want it to?
It can be so confusing and frustrating trying to work out why our body is behaving in certain ways, especially with sex, as it seems to be contradicting our thoughts or feelings. Here are 3 ways to understand arousal that may help you better understand yourself.
2 caveats:
1. Although these 3 models seem to work well for many neurotypical people, they don’t seem to be so good for neurodivergent folks.
2. For ace folks, sexual arousal may be a confusing issue if you do enjoy arousal but don’t want sex, with or without another person, or don’t want penetration. Or, you may prefer not to feel aroused at all. Wanting sensual pleasure without sexual arousal is a totally valid choice. Your body, your unique definition of pleasure, your choice.
Model 1: The Sexual Response Cycle
In the 1960s, Masters & Johnson mapped a 4-stage model to describe the human orgasm process, called the sexual response cycle. In order, the 4 stages are:
- arousal/excitement
- plateau
- orgasmic
- resolution.
Although this model has come under criticism since, it’s useful to allow us to explore different elements of sex and intimacy with broad brushstrokes.
For now, let’s focus on the first stage, excitement, which we commonly call arousal. Physically, signs of arousal can be increased breathing and heart rate and a rise in blood pressure and skin temperature. Typically, the nipples, penis, and clitoris become hard, the anus contracts, and the labia and vaginal walls lubricate. Sensory sensitivity increases.
Critics of Masters & Johnson have pointed out that this model might map arousal but doesn’t explain it or help us understand when it doesn’t work as expected. It also has orgasm as the ‘goal’ of arousal rather than one enjoyable element of many within the overall sexual experience. Another important point that’s missed out is that arousal is more than just a collection of physical responses. These points together lead to the development of the next model. This explores how the mental, emotional, and physical aspects of arousal are connected and what happens when something interrupts that flow.
Model 2: The Arousal Cycle
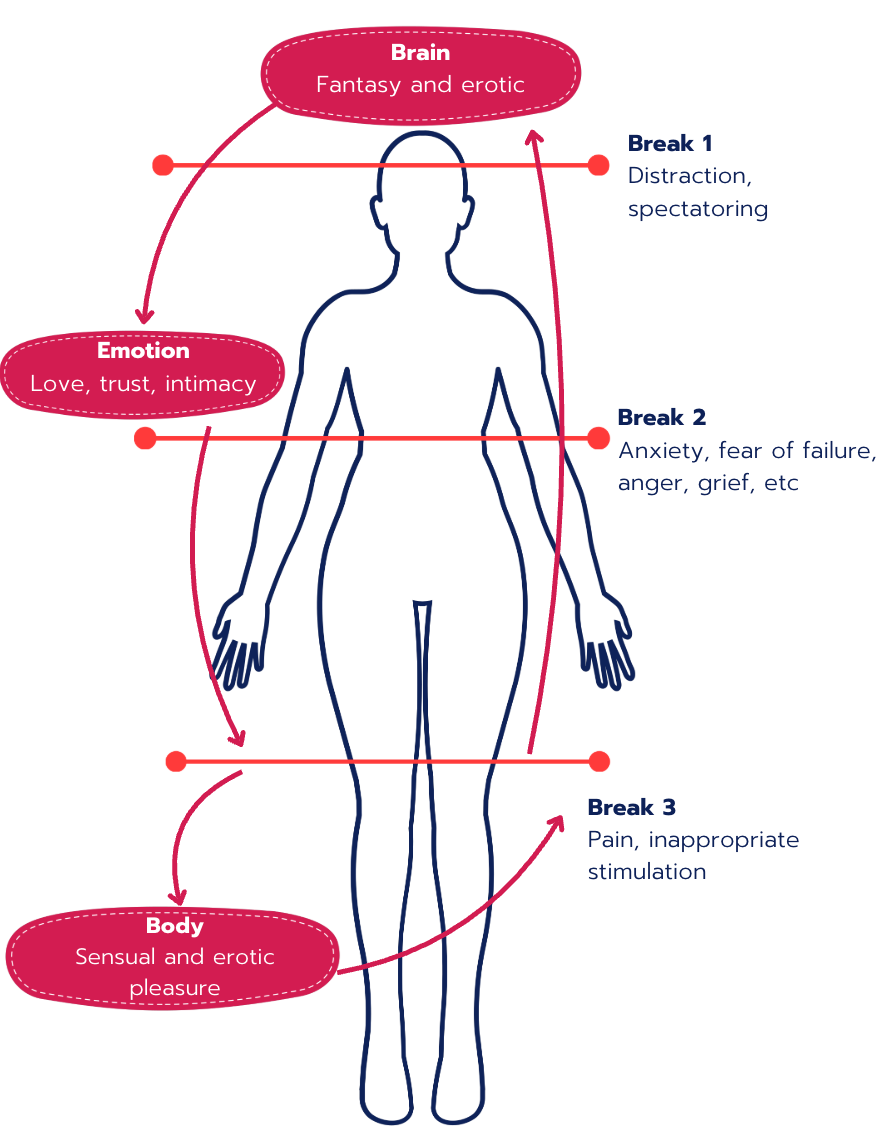
As you can see, on the left-hand side of the diagram, there are three originators of arousal: the brain/mind, the emotions/feelings, and the body.
Arousal can either originate in the body through physical stimulation, such as kissing and touching. Feeling loved and connected to someone can also feel sexually exciting and arousing. Arousal can start in the mind through imagination, such as fantasising or watching porn.
It can start in one, two, or all three areas simultaneously. The arousal in one area then flows into the other areas and builds up as the excitement circulates. Some people need all three areas stimulated all of the time, or some of the time, and other people only need one or two.
Most people have a preference for how they like to start the arousal process. This may be different when with a partner and when masturbating. The social stereotypes are that men prefer porn (mental) or touch (body), and women prefer connection (emotion).
- Is this true for you?
- Is it true for your partner(s)?
- How do you prefer being aroused, and does your partner know?
Breaking The Arousal Cycle
On the right-hand side of the diagram, there are 3 breakpoints, indicated with red lines.
On the mental level, this can be worrying about things to do or anything that keeps the person stuck in their head and not in their body, and/or connected to their partner, if they’re with someone else. Emotionally, we might struggle to feel aroused with a stranger (and possibly be demisexual) because there’s insufficient intimacy. I think we’ve all had occasions when we’ve been touched in ways that turn us off, or the person smells or tastes bad. Whatever the reason, a break anywhere in the cycle usually stops the whole cycle.
For some people, when the cycle has been broken, all the momentum drains away, but it can be restarted. This can be done immediately or takes a few minutes. For other people, that’s not an option, and they need to change activity and come back to sex another time, maybe another day.
- What tends to break your cycle?
- Is it something you do or your partner(s) does?
- What’s something you could do to reduce the chances of breaking your cycle?
Model 3: Nagoski's Brakes and Accelerators
The more complex idea of arousal having breaks and accelerators was popularised in the highly successful book, “Come as you are“, based on Kinsey Institute research from the 1990s. Sadly, there’s no diagram for this model. But there is a questionnaire you and your partner(s) can complete here. There is also a companion workbook.
Just as you can press on the accelerator in a car and it speeds up, so there are things we can do to increase our arousal. Our sexual accelerator is called the “Sexual Excitement System” (SES) and is primarily linked to the sympathetic nervous system. The break operates more through the parasympathetic nervous system and is called the “Sexual Inhibition System” (SIS). In order to get aroused, you need to increase the stimulation to the accelerator and decrease it on the brakes.
Interestingly, there are actually two types of breaks within our nervous system, much like a car. There’s the instant foot break, which is an immediate “no” that prevents us from getting aroused at inappropriate times. This type of break turns on when we’re concerned about the consequences of getting aroused or having sex at that time, along the lines of “what will my boss/parents/grandad think” or “I’m taking too long to orgasm”.
The other break is a slower, often chronic “no”. Much like driving with the handbrake on, you can get aroused, but it’ll be slower, less enjoyable, and you may struggle to climax. This break is typically related to fear of sexual performance and external factors, such as worrying about STIs or pregnancy.
If you’re neurodivergent and want to have another framework for understanding your personal sensory processing styles and sex, this article might help.
What If I'm... Broken?
If your arousal doesn't seem to work like any of these models, let me reassure you, you’re almost certainly not broken, and you are certainly not alone. The blanket clinical terms for a lack of arousal are called erectile dysfunction (ED) if you have a penis and sexual arousal disorder if you don’t. For example, in the US, an estimated 8 million people experience ED, so roughly 20% of the total population.
These conditions can be lifelong or arise at any time of life for a vast array of reasons. It may have emotional or psychological causes that are not directly related to a person’s relationship or sex life, such as work stress. It can be hormonal, or medications, such as SSRIs, can increase the chances of arousal problems.
You can significantly change arousal issues. You just need to find the right types of stimulation and remove things that are diminishing your arousal.
What If... You're Not Broken?
The good news is that there are tons of ways to get you and your arousal back on track. It’s heartbreaking to read that one study found over 75% of diagnosed ED cases go untreated. Shame or embarrassment shouldn't prevent you from seeking help.
Treatment can be a mixture of talk therapy, sex therapy, physical exercises, medication, and lifestyle changes. Sex therapy can radically improve your sex life by helping reframe sex as an enjoyable, intimate activity rather than a goal-oriented performance.
Seeking Help
I appreciate this is a long article – and it could have been much longer! But I wanted to help explain the different ways we can understand arousal. If you do struggle with arousal, you don’t need to suffer alone.
I encourage you to take the brave step and get in touch with a professional, such as your GP or a sexual health clinic. If you can afford private support, search for a sex therapist or sexologist. You may also enjoy my free 10-Step Guide to Prepare for Sex Therapy.
Tiga-Rose Nercessian (she/her), PhD Sex & Relationship Psychotherapist (UKCP, NCPS, COSRT Accredited) | Founder of Intimata | Specialising in Relationship Intelligence & Enhancement and Neurodivergent Intimacy.